Idiopathic Parkinson’s disease is a progressive neurodegenerative disorder characterized clinically by rigidity, tremor, and bradykinesia.
PHYSICAL FINDING AND CLINICAL PRESENTATION
- Tremor—typically, a resting tremor with a frequency of 4 to 6 Hz is often fi rst noted in the hand as a pill-rolling tremor (thumb and forefi nger), and can also involve the legs and lips. Tremor improves with purposeful movement, and usually starts asymmetrically.
- Rigidity—increased muscle tone that persists throughout the range of passive movement of a joint. This is also usually asymmetrical in onset.
- Akinesia, bradykinesia—slowness in initiating movement
- Masked facies—face seems expressionless, giving the appearance of depression. There is decreased blink and often excess drooling
- Gait disturbance (Figure 1)
- Stooped posture, decreased arm swing
- Difficulty initiating the first step; small shuffling steps that increase in speed (festinating gait). Steps become progressively faster and shorter while the trunk inclines farther forward.
- Other early complaints and findings include micrographia (handwriting becomes smaller) and hypophonia (voice becomes softer).
- Postural instability—tested by the pull test. Ask patient to stand in place with his or her back to the examiner. The examiner pulls the patient back by the shoulders; the proper response would be to take no or very few steps back without falling. Retropulsion is a positive test, as is falling straight back. This is not usually severe early. If falls and postural refl exes are greatly impaired early, then consider other disorders.
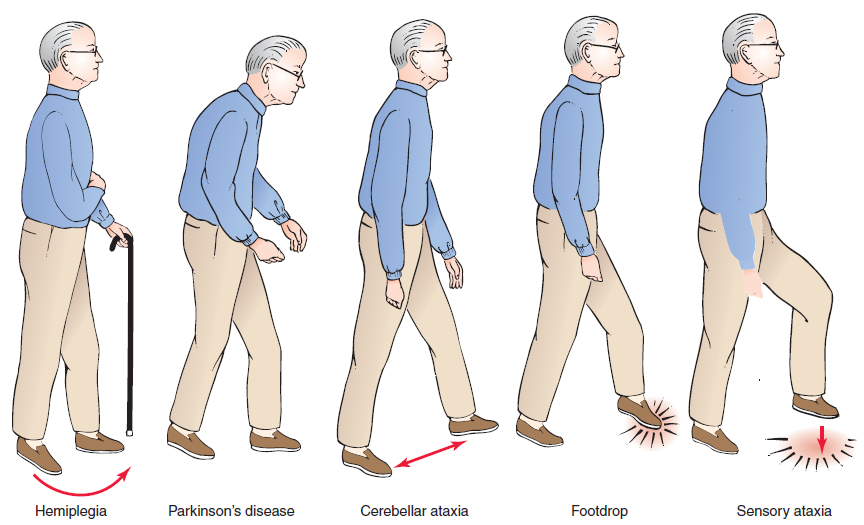 |
| Figure 1: Common types of gait abnormalities |
CAUSES
- Unknown
- Most cases are sporadic, with age being the most common risk factor, although there is probably a combination of environmental and genetic factors contributing to disease expression. There are rare familial forms with at least five different genes identified. The most well known is the parkin gene, which is a significant cause of early-onset autosomal recessive Parkinson’s disease and isolated juvenile-onset Parkinson’s disease (at or before age 20).
- A presumptive clinical diagnosis can be made based on a comprehensive history and physical examination. The combination of asymmetrical signs, resting tremor, and good response to levodopa best differentiates idiopathic Parkinson’s disease from other causes of parkinsonism (see “Differential Diagnosis” for PD).
- Multisystem atrophy—distinguishing features include autonomic dysfunction, (including urinary incontinence, orthostatic hypotension, and erectile dysfunction), parkinsonism, cerebellar signs, and normal cognition.
- Diffuse Lewy body disease—parkinsonism with concomitant dementia. Patients often have early hallucinations and fluctuations in levels of alertness and mental status.
- Corticobasal degeneration—often begins asymmetrically with apraxia, cortical sensory loss in one limb, and sometimes alien limb phenomenon.
- Progressive supranuclear palsy—tends to have axial rigidity greater than appendicular (limb) rigidity. These patients have early and severe postural instability. A hallmark is supranuclear gaze palsy that usually involves vertical gaze before horizontal.
- Essential tremor—bilateral postural and action tremor.
- Secondary (acquired) parkinsonism
- Postinfectious parkinsonism—von Economo’s encephalitis
- Parkinson’s pugilistica—after repeated head trauma
- Iatrogenic—any of the neuroleptics and antipsychotics. The high potency D2-blocker neuroleptics are most likely to cause parkinsonism.
- Toxins (e.g., MPTP, manganese, carbon monoxide)
- Cerebrovascular disease (basal ganglia infarcts)
- CT has almost no role in investigations. MRI of the head may sometimes distinguish between idiopathic Parkinson’s disease and other conditions that present with signs of parkinsonism.
- For management and treatment please read full information:
- Ferri's Clinical Advisor
- American Family Physicians Journal
- The Washington Manual
- Medscape Reference
- The New England Journal of Medicine





0 comments:
POST A COMMENT